About this project
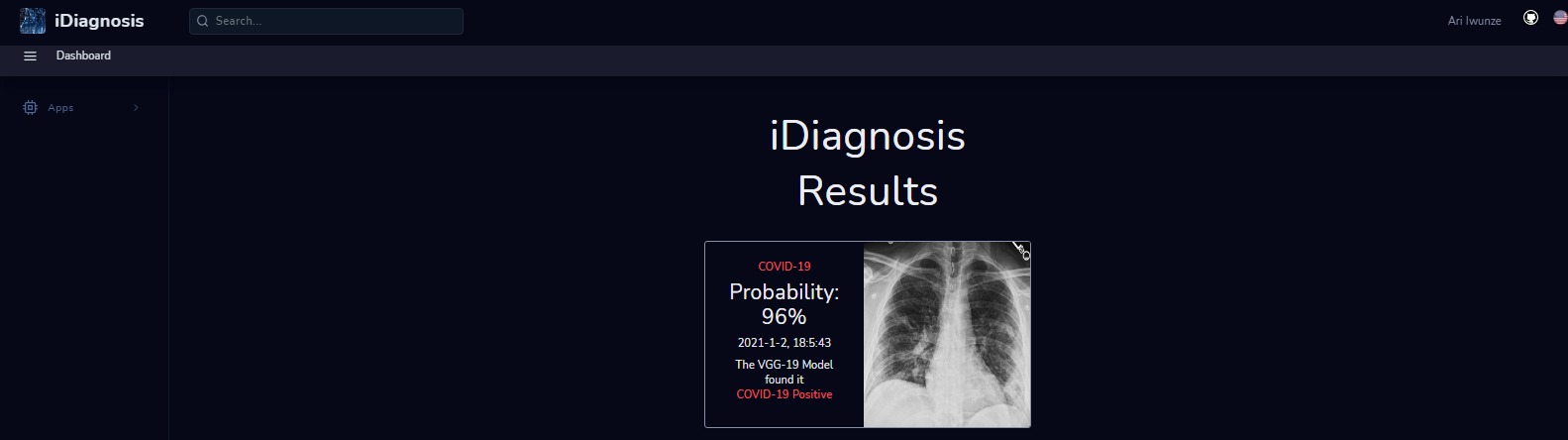
A web application that uses computer vision analysis to diagnose and distinguish between Pneumonia and COVID-19 using the VGG19 deep learning algorithm. The purpose is to build a classifier that can correctly distinguish between Pneumonia and Covid-19, motivated by the 100,000 deaths per year due to misdiagnosis of pneumonia and the fact that pneumonia is the leading cause of fatality in children under 5.
Key features
- 01The network used is VGG19 due to its strong accuracy on image classification problems.
- 02Pre-trained weights are loaded with include_top=False so the final 1000-class layer is dropped.
- 03New top layers are added for binary classification (Pneumonia vs Covid-19).
- 04ImageDataGenerator augments training (batch size 32, image size 64x64).
Methodology & results
Purpose
The goal is a classifier that can correctly distinguish between pneumonia and COVID-19 on a chest X-ray. Why lung diseases in particular:
- Roughly 100,000 deaths per yearare attributable to misdiagnosed pneumonia. Wrongful diagnosis is life-threatening because it delays treatment — especially when the underlying condition is a more aggressive respiratory infection like COVID-19.
- Pneumonia accounts for roughly 1 in 6 childhood deaths globally, making it the leading cause of fatality in children under five.
- The US pneumonia mortality rate sits near 10 per 100,000 — typical of developed economies. In much of sub-Saharan Africa the rate is closer to 100 per 100,000, an order of magnitude higher, reflecting how much room a cheap screening tool has to make a difference.
Model
The backbone is VGG19— well-established on image classification and cheap to fine-tune. ImageNet weights are loaded with include_top=False, dropping the final 1,000-class head that would otherwise be useless for a two-class problem. The input layer is also swapped to accept custom image dimensions. On top of the frozen convolutional stack sit a small dense head and a binary softmax.
Training data flows through ImageDataGeneratorwith a batch size of 32 and images resized to 64×64. Three separate binary classifiers are trained: COVID-19 vs. Normal, Pneumonia vs. Normal, and a multi-class Pneumonia vs. COVID-19 head.
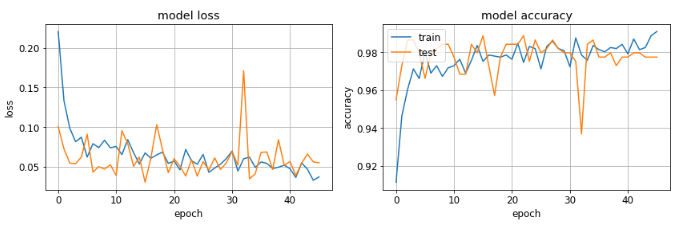
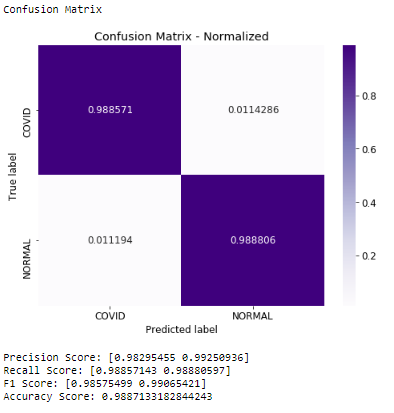
COVID-19 vs. Normal
Accuracy sits at 99%; recall on the positive class is also 99%. Recall is the metric that matters most here: in a screening context, a false negative — missing a real COVID case — is far more costly than a false positive that prompts a second look.
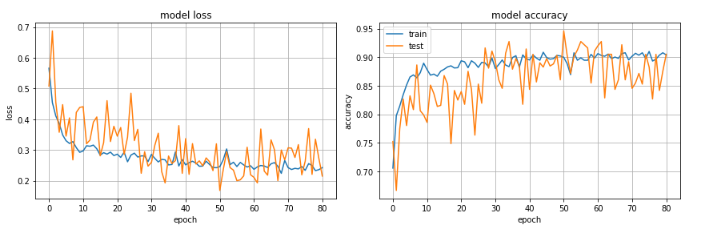
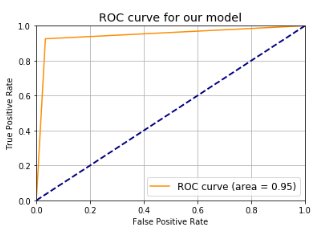
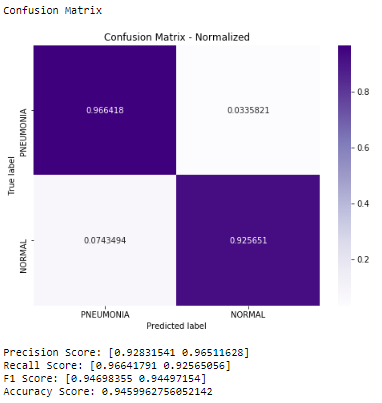
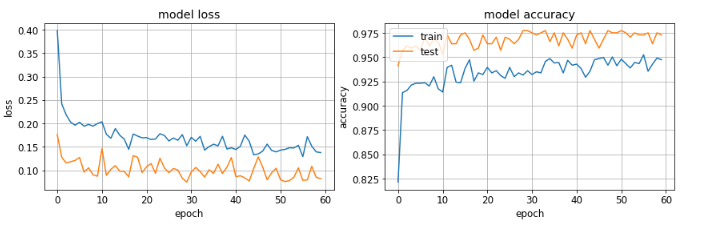
Pneumonia vs. Normal
Accuracy: 94%. Recall on pneumonia: 95%. AUC: 0.90. Loss on the held-out set: 0.17. The pneumonia task is genuinely harder than the COVID task — pneumonia opacities are more diffuse and the class boundary less sharp — and the numbers reflect that.
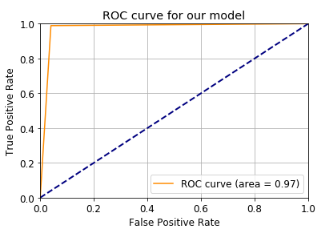
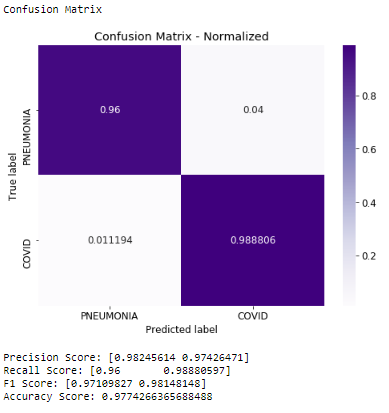
Pneumonia vs. COVID-19
The multi-class head separates the two diseases directly. Loss drops to 0.02, AUC climbs to 0.93, and recall on the COVID class reaches 100%. The specialised binary COVID and pneumonia models still contribute value — they can serve as sanity checks on the multi-class output — but the multi-class model is the one you would deploy.
Recommendation
Against a plain baseline the VGG19 fine-tune is roughly 26% better at correctly diagnosing COVID in the binary task and roughly 15% better in the multi-class task. Two improvements are worth wiring in before production:
- Dropout before the final dense layer. Half the activations from a 512-unit dense layer are dropped during training to keep the model from memorising the small dataset.
- Multi-class head as the primary output. The binary models are retained only for internal cross-checks.
Future work
- Other lung diseases. Extend the classifier to tuberculosis, bronchitis, and other pathologies so a single tool can triage a broader differential.
- Region localisation.Move from image-level classification to lesion detection — where in the lung the infection sits, not just whether it’s present.
- More data, deeper tuning. Unfreeze more of the VGG19 base and train against a larger, more diverse cohort to shrink the domain-shift gap between hospitals and X-ray hardware.